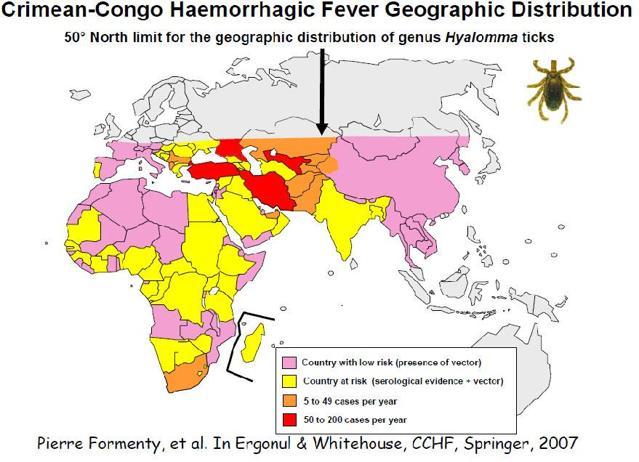
Economics of Crimean-Congo Fever
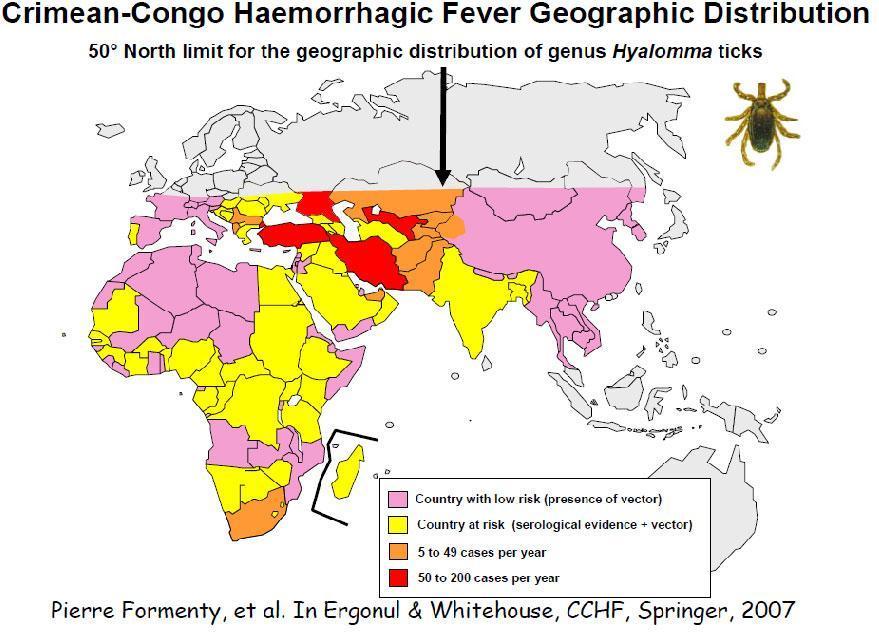 With the advent of summer, Crimean-Congo Hemorrhagic Fever (CCHF) cases have started to appear in Turkey once again.
With the advent of summer, Crimean-Congo Hemorrhagic Fever (CCHF) cases have started to appear in Turkey once again.A two-day conference on infectious diseases in Istanbul, which is ending today, has made me wonder why there is no vaccine for CCHF. A multinational pharmaceutical executive told me they simply would not be able to recoup their expenses since the market for such a vaccine is too small. There are only a handful of countries with more than five cases per year, whose combined GDP is less than Germany’s.
Economist Michael Kremer of Harvard University saw this problem a decade ago. His solution was that developed countries could make a binding commitment to buy a vaccine once it is developed. While this “advance purchase commitment” was proposed for deadlier diseases like AIDS, it could certainly work for CCHF as well.
Turkey is rich enough to make such a commitment by itself. Besides, while the disease appeared here much later than in other countries, Turkey accounts for nearly half of the cases in the world, with 7000 occurrences in the last decade, 400 of which were fatal.
But Önder Ergönül of Koç University, one of the leading CCHF researchers in the world, noted during a chat on Friday, that it would take time to develop a vaccine. He highlighted the importance of early diagnosis and treatment. There are drugs that have been shown to be effective against CCHF, so he recommends their administration even in cases where infection is probable, but not certain.
Take the case of nurse Kübra Yazım who in 2009 became infected from a needle at Samsun’s 19th May University and then died. She was not given any medicine. Interestingly, there are several academics who believe existing drugs are ineffective against CCHF.
To judge for myself, I read a paper written by the proponents of this view. I am no medicine man, but calling the statistical methodology of the paper “flawed” would be an understatement. Another paper that argues against the use of drugs has been subject to severe criticism, not only on statistical but also ethical grounds.
It is true that these drugs are very expensive, but the government has been very successful at getting costly vaccines at dirt-cheap prices, so I could not understand this resistance, at least until I found out that some pharmaceutical companies produce them while others don’t. It seems CCHF treatment has fallen prey to the “battle of the pharmaceuticals”.
One could also argue that there isn’t definitive evidence on the efficacy of existing drugs. While Centers for Disease Control and Prevention notes that one particular drug “has been used in the treatment of CCHF patients reportedly with some benefit,” recent papers are arguing for randomized controlled trials.
In fact, I was told that the Ministry of Health is considering exactly that. That immediately brought to my mind the infamous Tuskegee syphilis experiment, in which African American patients were not administered penicillin even after the drug had been validated as an effective cure for the disease.
It would be great to see a “Turkey CCHF experiment” make it to case studies in ethics classes of major medical schools.









